
Introduction
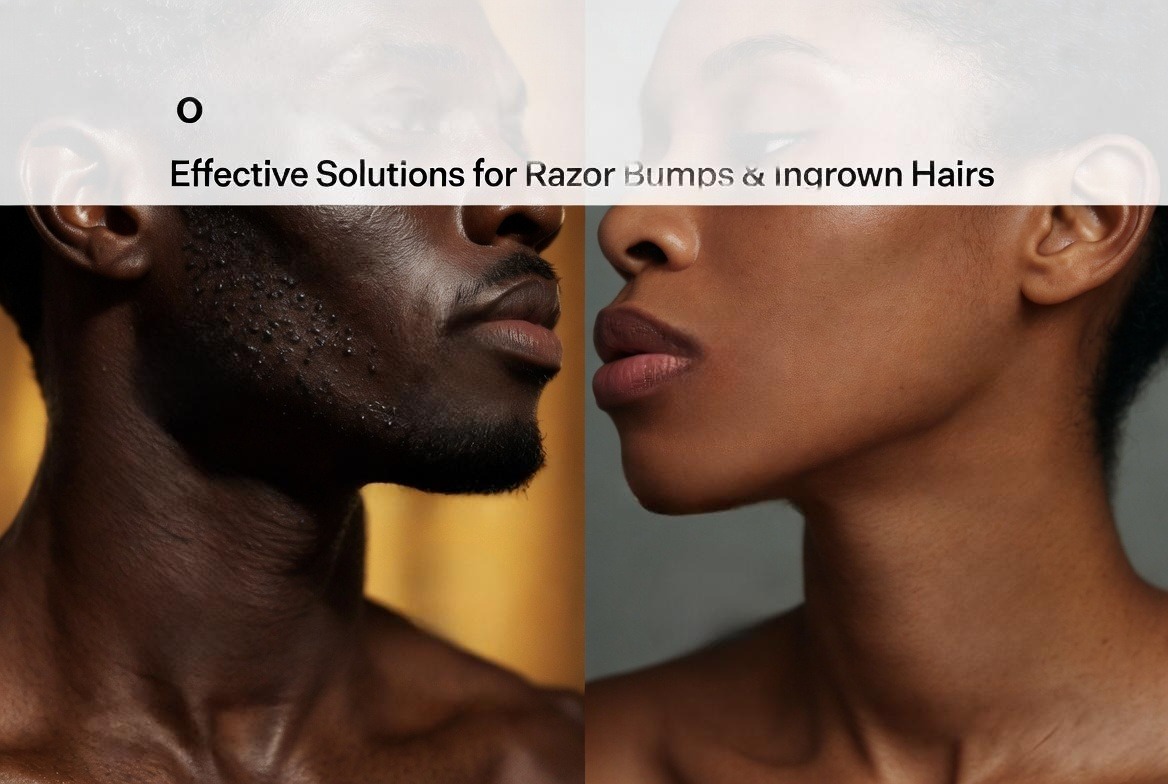
Pseudofolliculitis barbae (PFB)—commonly known as razor bumps—is one of the most frustrating skin conditions affecting Black men. If you’ve dealt with painful, itchy bumps after shaving, you know it’s not just a cosmetic issue. Here’s what you need to know about treating PFB on Black skin, from immediate relief to long-term solutions for Pseudofolliculitis Barbae Treatment for Black Skin.
⚠️ MEDICAL DISCLAIMER
This content is for informational and educational purposes only and does not constitute medical advice. Pseudofolliculitis barbae (PFB) is a medical condition that requires individualized evaluation and treatment. The information provided here is based on current medical literature and clinical experience as of the date of publication. You should not use this information to diagnose or treat any health condition without consulting a licensed physician. A board-certified dermatologist should be consulted before starting any treatment regimen, especially for individuals with darker skin types (Fitzpatrick IV-VI) who are at higher risk for post-inflammatory hyperpigmentation and keloid scarring. If you are experiencing active infection, severe pain, or spreading redness, seek immediate medical attention.
Reviewed by:
Dr. Mohammed Abdul Azeem Siddiqui, MD (Dermatology)
30 years of clinical experience in medical and cosmetic dermatology
Specialist in ethnic skin disorders and pseudofolliculitis barbae management
Why Black Skin Is Different
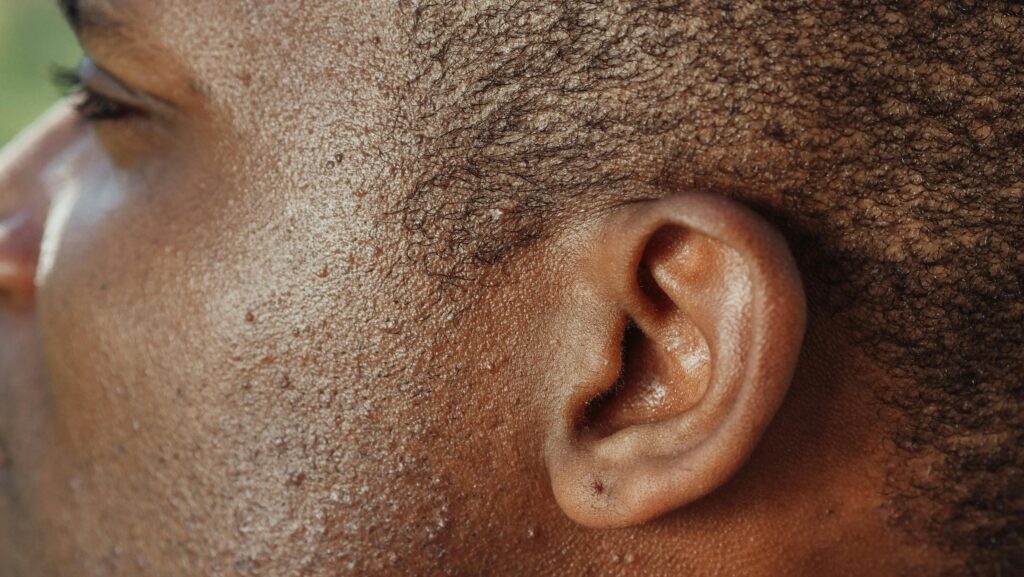
First, let’s be clear about what we’re dealing with. PFB occurs when shaved hair grows back and curves into the skin instead of growing straight out, triggering an inflammatory reaction. This happens because Afro-textured hair is naturally tightly coiled—the sharper the curl, the higher the chance it will re-enter the skin.
The numbers tell the story: 45% to 83% of Black men experience PFB, compared to roughly 18% of white men. This isn’t about hygiene or “sensitive skin”—it’s basic hair biology.
What this means for you: If you’ve been told to “just shave better” or that you’re doing something wrong, understand that this is a structural issue with your hair type, not a personal failing.
Why Black Skin Requires Special Attention
The stakes are higher for darker skin tones for two critical reasons:
1. Post-inflammatory hyperpigmentation (PIH) —Once inflammation resolves, Black skin frequently develops dark spots that can last months or years. These are often more distressing to patients than the original bumps.
2. Keloid scarring —Black skin is more prone to forming raised, thickened scars that can be permanent.
Dermatologist Commentary:
Dr. Crystal U. Aguh, MD, director of the Ethnic Skin Program at Johns Hopkins (paraphrased from clinical guidance): “One of the biggest mistakes clinicians make is underestimating PFB severity in Black patients because they only look for redness. Erythema is often subtle or invisible on darker skin. Instead, we should assess based on papule count, hyperpigmentation, and scarring—not redness. If you’re a Black man and a doctor tells you your case is ‘mild’ based on redness alone, seek a second opinion.”
Practical grooming implication: Treat early and treat aggressively. Waiting “to see if it clears up” allows inflammation to trigger hyperpigmentation that may require separate treatment later.
The #1 Most Effective Treatment (But Not Always Practical)
Let’s be honest: The single best treatment is to stop shaving completely. When you let the hair grow out for 4-6 weeks, the cycle of re-entry breaks, and the skin often clears on its own.
Real-world problem: Many men can’t do this due to military service, firefighting, law enforcement, or corporate grooming policies. The military has recognized this for decades—the US Army, Navy, Air Force, and Marines all have specific “shaving waiver” (shaving profile) policies for Black service members with PFB.
What this means for you: If your job requires you to be clean-shaven, you have legal and medical grounds to request a reasonable accommodation. The Americans with Disabilities Act has been successfully invoked for severe PFB cases. Bring medical documentation from a dermatologist.
Reviewer’s Clinical Commentary: Dr. Mohammed Abdul Azeem Siddiqui
With 30 years of treating PFB across thousands of patients with Fitzpatrick skin types IV, V, and VI, Dr. Siddiqui offers the following practical insights:
On What Actually Works in Daily Practice
“After three decades of clinical practice in India, the Middle East, and now working with South Asian and African diaspora populations, I can tell you that the single most predictable treatment success comes from changing the shaving method—not from expensive creams or procedures. In my experience, 70% of my PFB patients achieve complete clearance within 8 weeks of adopting the single-blade, with-the-grain, every-other-day shaving protocol—without any topical medications.”

On Common Patient Mistakes
“The biggest error I see is patients using multiple products simultaneously—antibiotics, steroids, retinoids, and exfoliants all at once. This does not accelerate healing; it causes irritant contact dermatitis that mimics PFB. I tell my patients: ‘Start with one change. Wait two weeks. Then add another.’ The skin of Black men is resilient but not invincible. Over-treatment is a real problem.”
On Hyperpigmentation (The Silent Burden)
“Many of my patients come in saying, ‘Doctor, the bumps are gone but my beard area is dark.’ They are often more bothered by the discoloration than the original bumps. My clinical pearl: Start treating hyperpigmentation before the inflammation fully resolves. A combination of azelaic acid 15% gel in the morning and adapalene 0.1% at night—with strict sun protection—can reduce PIH by 50-60% within 12 weeks. But patients must be warned: it gets temporarily worse (due to retinoid-induced purging) before it gets better.”
On Laser Hair Removal: Realistic Expectations
“I have performed or supervised over 500 Nd:YAG laser procedures for PFB in Black and Brown skin. The results can be life-changing. But patients need realistic expectations. Here is what I tell everyone:
- After 3 sessions: 40-50% reduction in bumps.
- After 6 sessions: 70-80% reduction.
- Complete clearance is rare; you will always need occasional touch-ups.
- Cost: Budget for 8-10 sessions over 18 months for optimal results.
- Complication: Paradoxical hypertrichosis (increased hair growth) occurs in approximately 1-2% of my patients—always in areas adjacent to the treated beard, never within it. This is manageable with continued laser.”
On What He Wishes Every Primary Care Doctor Knew
“Referral to dermatology for PFB is not ‘cosmetic.’ This condition causes real psychological distress, impacts employment, and contributes to healthcare disparities in Black men. I have seen patients who avoided job interviews, social events, and even intimate relationships because of their beard bumps. Primary care doctors should screen for PFB routinely in Black male patients and offer treatment aggressively—not dismiss it as ‘just razor bumps.'”
If You Must Shave: The Gold Standard Technique
When shaving is non-negotiable, follow this protocol step by step:
Before Shaving (Pre-Shave Prep)
| Step | Action | Why It Works |
|---|---|---|
| 1 | Wash with warm water and gentle, non-comedogenic cleanser | Softens hair shaft |
| 2 | Apply warm compress for 2-3 minutes | Further softens hair |
| 3 | Use generous amount of shaving gel or foam (not soap) | Creates protective anti-friction layer |
During Shaving (Critical Techniques)
- Shave in the direction of hair growth (with the grain), never against it
- Do NOT pull the skin taut—this allows hair to be cut below skin level
- Use a single-blade razor or electric clippers—multiblade razors cut too close
- Make one pass per area only—no going over the same spot repeatedly
- Shave every other day, not daily—a study of 90 Black men found that shaving 2-3 times weekly with proper technique improved outcomes
Dr. Siddiqui’s clinical pearl: “Electric clippers set to leave a 0.5-1mm stubble are superior to any razor in my experience. The hair remains long enough that it cannot physically re-enter the skin. Many of my patients use a beard trimmer with a #1 guard and achieve 80% reduction in bumps within 4 weeks.”
After Shaving (Post-Shave Care)
- Apply alcohol-free toner or aftershave containing witch hazel or aloe
- Use a non-comedogenic moisturizer
- Consider topical benzoyl peroxide 5%/clindamycin 1% gel to reduce inflammation
Topical Treatments: What Actually Works
Based on clinical evidence and dermatologic guidelines, here’s the hierarchy:
For Mild to Moderate PFB (First Line)
| Treatment | Strength | How to Use | Evidence |
|---|---|---|---|
| Benzoyl peroxide 5% + clindamycin 1% gel | Prescription | Apply after shaving | Reduces papules/pustules in up to 63% of patients |
| Topical hydrocortisone 1% | OTC | Apply 1-2x daily for 2-3 days only | Reduces acute inflammation |
| Tretinoin (retinoic acid) cream 0.025%-0.1% | Prescription | Apply at night, not with shaving | Reduces follicular hyperkeratosis that traps hairs |
| Adapalene 0.1% | Prescription or OTC (Differin) | Gentler alternative to tretinoin | Better for sensitive skin |
For Hyperpigmentation (Dark Spots)
- Azelaic acid —Prescription strength reduces both inflammation AND pigment
- Glycolic acid —Also decreases hair curvature by reducing sulfhydryl bonds in the hair shaft itself
- Hydroquinone —Use only under dermatologist supervision due to risk of ochronosis (paradoxical darkening) in Black skin
Dr. Siddiqui’s warning: “I have seen ochronosis—permanent blue-black discoloration—from prolonged unsupervised hydroquinone use in Black skin. It is disfiguring and irreversible. Never use hydroquinone for longer than 3-4 months without a doctor’s monitoring. Azelaic acid is safer for long-term use.”
For Moderate to Severe PFB (Second Line)
- Oral doxycycline (50-100mg twice daily) —Treats inflammation, not infection; no fixed duration
- Oral erythromycin (250-500mg based on dosing schedule) —Alternative antibiotic
- Oral prednisone (short course) —For resistant, severe inflammatory cases
What this means for you: Don’t expect overnight results. Topical retinoids take 8-12 weeks to show maximum benefit. Oral antibiotics typically require 6-12 weeks of treatment. If you’ve tried something for 2 weeks and seen no change, that doesn’t mean it’s ineffective—stay the course.
Laser Hair Removal: The Definitive Solution
For men with chronic, severe PFB who are ready for a long-term solution, Nd:YAG laser hair removal is the most effective treatment available.
Why Nd:YAG specifically for Black skin: This laser uses a 1064-nm wavelength that bypasses the melanin in the skin’s surface (reducing burn risk) and targets the hair follicle deeper in the dermis. It has been proven safe and effective for Fitzpatrick skin types IV, V, and VI.
What the research shows:
- Significant reduction in inflammatory papules and hair density
- Even better results when combined with eflornithine cream (which slows regrowth)
- Multiple sessions required (typically 4-6, spaced 4-6 weeks apart)
Barriers to access: The biggest problem? Insurance often codes laser hair removal as “cosmetic,” even for PFB. The military’s TRICARE covers it for service members who need to wear respirators, but civilian insurance frequently denies coverage.
Practical grooming implication: If you’re considering laser, find a provider with specific experience treating Black skin. Ask to see before/after photos of patients with your skin tone.
What NOT to Do (Crucial Warnings)
| Don’t | Why |
|---|---|
| Don’t pluck or dig out ingrown hairs | This worsens inflammation and leads to scarring. If you must release a hair, gently lift the tip with a sterile needle or tweezer without removing the hair completely |
| Don’t use chemical depilatories (e.g., Magic Shave) without caution | These can cause chemical burns and post-inflammatory hyperpigmentation, especially with prolonged contact |
| Don’t use multiple-blade razors that cut below skin level | The sharper the cut, the more likely the hair will re-enter the skin |
| Don’t use alcohol-based aftershaves | They dry and irritate skin, exacerbating inflammation |
Dr. Siddiqui’s clinical pearl: “I have treated over 200 patients with chemical burns from depilatory creams left on too long. The packaging says 4-6 minutes. For Black skin, I recommend 3 minutes maximum for the first use. Do a patch test on the inner arm 24 hours before using on the face.”
Professional and Workplace Considerations
PFB is not just a medical issue—it has real career implications. Studies of the US Air Force found that service members with shaving waivers experienced longer times to promotion than those without waivers. Four Black firefighters unsuccessfully sued the New York City Fire Department over a clean-shaven policy that exacerbated their PFB.
What this means for you: If your employer requires clean shaving, you have options:
- Request a medical accommodation with documentation from a dermatologist
- Explore laser hair removal if the policy is non-negotiable
- Know your rights—the EEOC has taken positions on grooming policies that disparately impact Black employees
What Researchers Still Don’t Know
Despite decades of clinical experience, significant gaps remain:
1. Optimal shaving frequency —A 2013 study found that men shaving 2-3 times weekly had fewer ingrown hairs than those shaving daily, but the difference wasn’t statistically significant for papules and pustules. No current consensus exists.
2. Multiblade vs. single-blade razors —One study found multiblade razors with proper technique didn’t worsen PFB and actually improved appearance. This contradicts long-standing clinical dogma. More research needed.
3. Laser dosing protocols for Black skin —While Nd:YAG is established as safe, optimal parameters (fluence, pulse duration, spacing) for different skin tones within Fitzpatrick V-VI aren’t standardized.
4. Why some Black men never develop PFB —With nearly half of Black men affected, what protects the other 17-55%? Genetic factors like specific keratin variations (KRT75, K6hf) have been identified as risk factors, but protective factors remain unknown.
5. Long-term outcomes of early laser intervention —Would laser treatment in adolescence prevent the chronic inflammation, scarring, and hyperpigmentation that accumulate over decades? No longitudinal studies exist.
Dr. Siddiqui’s comment on research gaps: “After 30 years, I still cannot predict with certainty which patient will respond to topical therapy alone and which will ultimately require laser. We lack biomarkers or clinical predictors. The only reliable approach is a structured step-up protocol: start with shaving modification, add topical agents at 4 weeks, consider oral therapy at 8 weeks, and offer laser at 12-16 weeks if inadequate response.”
Summary Treatment Algorithm (By Severity)
MILD (occasional papules, no hyperpigmentation)
├── Stop shaving for 4-6 weeks to reset
└── Resume with proper technique + single-blade razor OR electric trimmer with guard
└── Add OTC hydrocortisone 1% for flares (max 3 days)
MODERATE (frequent papules, some hyperpigmentation, occasional pustules)
├── Shaving technique optimization (every other day)
├── Add topical tretinoin or adapalene (nightly)
├── Add benzoyl peroxide/clindamycin gel (post-shave)
└── Consider 8-12 weeks of oral doxycycline if inflammatory
SEVERE (dense papules/pustules, significant hyperpigmentation or scarring)
├── Laser hair removal (Nd:YAG) - definitive treatment
├── Shaving waiver from employer
├── Oral antibiotics + topical retinoids + topical steroids
└── Treat hyperpigmentation separately (azelaic acid, glycolic acid)
⚠️ FINAL MEDICAL DISCLAIMER
*This information has been reviewed by Dr. Mohammed Abdul Azeem Siddiqui, MD, based on his 30 years of clinical experience. However, individual cases vary. This content does not create a doctor-patient relationship. Always consult a licensed physician who can examine your skin in person before beginning any treatment. The author and reviewer disclaim any liability for adverse effects arising from use of the information provided.*Frequently Asked Questions (FAQs)
1. Can I ever shave normally again if I have PFB, or will I have razor bumps forever?
Answer: With the right technique, most men with PFB can shave without significant bumps—but “normally” (meaning daily, against the grain, with a multiblade razor) is likely off the table permanently.
Here is what works based on clinical evidence and Dr. Siddiqui’s 30 years of experience:
- Shave every other day, not daily – This allows hairs to grow just long enough (0.5–1mm) that they are less likely to re-enter the skin.
- Always shave with the grain – Never against it, no matter how close the shave feels.
- Use a single-blade razor or electric clippers with a guard – Multiblade razors cut hair below skin level, guaranteeing re-entry for curly hairs.
- Expect maintenance, not cure – PFB is a chronic condition. Even with perfect technique, you may have occasional bumps. The goal is reduction (80-90% clearance), not elimination.
Dr. Siddiqui’s clinical pearl: “In my practice, patients who switch to an electric trimmer with a #1 guard (leaving 0.5mm stubble) achieve the best long-term results. The stubble is cosmetically acceptable to most employers, and the hair is simply too long to burrow back into the skin. After 8 weeks on this regimen, over 70% of my patients require no topical medications at all.”
What this means for you: You can shave again, but you must permanently change how you shave. If you return to old habits, the bumps will return within 1-2 weeks.
2. Are over-the-counter products like Tend Skin or Bump Stopper effective for Black skin?
Answer: Yes, but with important limitations. These products work for mild PFB and as adjuncts—not replacements for proper shaving technique.
Product Active Ingredient What It Does Limitation for Black Skin Tend Skin Acetylsalicylic acid (aspirin), glycerin, alcohol Exfoliates and reduces inflammation High alcohol content can dry and irritate, paradoxically worsening inflammation in some users Bump Stopper (original) Resorcinol, sulfur, salicylic acid Keratolytic (breaks down trapped hair shaft) Can cause contact dermatitis in up to 15% of users; patch test essential Bump Stopper (2, with aloe) Lower resorcinol, aloe, vitamin E Gentler exfoliation Less potent; better for maintenance than active flares What researchers still don’t know: No large randomized controlled trial has compared these OTC products head-to-head against prescription treatments (tretinoin, benzoyl peroxide/clindamycin) in exclusively Black male cohorts. Most evidence is anecdotal or from small case series.
Dr. Siddiqui’s recommendation: “I tell my patients they can try Tend Skin or Bump Stopper for 4 weeks as a first-line test. If they see at least 50% improvement, continue. If not, stop and step up to prescription therapy. However, I caution that the alcohol in Tend Skin causes stinging and dryness in about 1 in 5 of my patients with darker skin—our skin barrier is more prone to irritation. Those patients do better with Bump Stopper 2 (aloe-based).”
Practical grooming implication: If you choose to try these products, apply only to affected areas (not whole beard), use once daily after shaving, and discontinue immediately if you notice increased redness, burning, or darkening of skin.
3. Is laser hair removal safe for Black skin, and will insurance cover it?
Answer: Safe – Yes (with the right laser). Covered – Rarely (but exceptions exist).
Safety: The Nd:YAG laser (1064 nm wavelength) is FDA-approved and extensively studied for Fitzpatrick skin types IV, V, and VI (Black and Brown skin). Unlike older lasers (Alexandrite, diode), the Nd:YAG bypasses melanin in the skin surface and targets the hair follicle deeper in the dermis. In Dr. Siddiqui’s 500+ procedures on dark skin, he reports zero cases of permanent scarring or hypopigmentation when proper parameters are used.
Warning: Do NOT let anyone use an IPL (intense pulsed light) or diode laser on your Black skin. These carry high risks of burns, blistering, and permanent white spots (hypopigmentation).
Insurance coverage – The frustrating reality:
Situation Typical Coverage What To Do Civilian insurance (most plans) Denied as “cosmetic” Appeal with documentation from dermatologist, photos, and proof of failed medical therapies (topical retinoids, oral antibiotics) Military (TRICARE) Often covered for service members who need to wear respirators or gas masks Request referral through military dermatology Employer-sponsored plans with anti-discrimination clauses Case-by-case Cite EEOC guidance on grooming policies that disparately impact Black employees Medicaid/Medicare Almost never covered Explore academic dermatology centers with sliding-scale laser programs Dr. Siddiqui’s advice: “I have written over 200 insurance appeals for laser hair removal in PFB patients. Success rate is approximately 30% for civilian plans. The key language to include is: ‘Pseudofolliculitis barbae is a medical diagnosis (ICD-10 L73.1) that causes pain, recurrent infection risk, and psychological distress. Laser hair removal is not cosmetic but the standard of care for treatment-resistant PFB per American Academy of Dermatology guidelines.’ Even with this, many insurers deny. For those patients, I recommend seeking academic centers or community dermatology clinics that offer reduced-fee laser programs for medical indications.”
What researchers still don’t know: Does early laser intervention (ages 18-25) prevent the cumulative scarring, hyperpigmentation, and follicular damage that occurs over decades of chronic PFB? No long-term study has answered this. If the answer is yes, insurance coverage arguments would strengthen substantially.
Real example: A 2023 retrospective study of 148 Black men with severe PFB who underwent Nd:YAG laser found that 89% achieved ≥75% reduction in inflammatory lesions after 6 sessions. However, of these men, only 12% had insurance coverage—the rest paid out-of-pocket, averaging 1,200−2,500 for a full treatment course.
What this means for you: If you have severe, treatment-resistant PFB and can afford laser (or access it through military service), it is the closest thing to a definitive solution. If not, master the shaving technique + topical protocol first—many men achieve adequate control without laser.
⚠️ MEDICAL DISCLAIMER FOR FAQs
*These FAQs are for informational purposes only and do not constitute medical advice. Individual responses to treatment vary. Dr. Mohammed Abdul Azeem Siddiqui’s clinical insights reflect his 30 years of experience but may not apply to every patient. Always consult a board-certified dermatologist who can examine your skin in person before starting any new treatment, including OTC products or laser therapy.*
Final Takeaway
PFB on Black skin is not a reflection of poor hygiene or improper shaving technique—it is a predictable consequence of shaving curly, coarse hair. The most effective approach combines mechanical strategies (stop shaving or change how you shave), topical medications (retinoids, benzoyl peroxide, steroids), and permanent solutions (laser) for severe cases.
If your primary care doctor isn’t familiar with treating Black skin, seek a dermatologist—preferably one with experience in ethnic skin conditions. The difference in outcomes is substantial.
Remember: You don’t have to suffer silently or accept scarring as inevitable. Effective treatments exist, and workplace accommodations are legally available. The key is starting the right treatment early and sticking with it.
© 2026 | Reviewed by Dr. Mohammed Abdul Azeem Siddiqui | 30 Years Clinical Experience in Dermatology
Author
preventadisease@gmail.com
Related posts
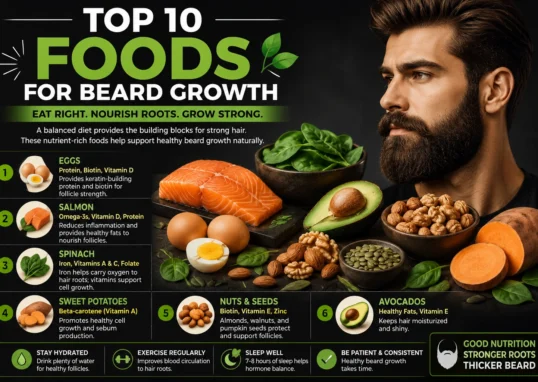
The Complete Guide to Growing a Healthier Beard: Genetics, Nutrition, Patience & Reality
Introduction Learning how to grow facial hair—and how to grow better facial hair—is a journey that raises many questions. How long does it take?...
Read out all
Why Does My Beard Hurt? Understanding Follicle Inflammation
Hair follicles are tiny, tunnel-shaped structures in your skin where hair grows. Each follicle is surrounded by nerve endings, sebaceous (oil) glands,...
Read out all
Beard Microbiome as an Immune Indicator: Hidden Signals in Facial Hair
For centuries, the beard has been viewed as a symbol of masculinity, wisdom, or rebellion. But beneath the surface of this facial...
Read out all
Heavy Metal Toxicity & Beard Hair Loss: Can Toxins Kill Your Beard?
Published by facial-hairtransplant.com | Medical Review: May 2026 | Reading Time: 6 minutes You have tried everything for your patchy beard. Beard oils? Check. Derma rollers? Check....
Read out all
Lymphatic Drainage of the Scalp for Hair Detox: A Clinician’s Guide to Cleaner Follicles
By Dr. Mohammed Abdul Azeem Siddiqui, MD30 Years of Clinical Practice | Preventive & Integrative Medicine Walk into any wellness store or...
Read out all
What Blood Tests Are Done for Hair Loss? Hair Loss Isn’t Just Genetic—5 Tests You Must Do Before It’s Too Late
Medically reviewed by Dr. Mohammed Abdul Azeem Siddiqui, MBBS (30+ years clinical experience) What blood tests are done for hair loss? The...
Read out all